NCERT Solutions of Class 11 Chapter 14 Breathing and Exchange of Gases
Last Updated :
02 Jun, 2023
NCERT Solutions for class 11 chapter-14 Breathing and Exchange of gases. The chapter on breathing and the exchange of gases is important for students approaching the exams. This article introduces NCERT solutions designed to help students explain the concepts of further learning and how to write to get good grades on exams. The solutions are presented in very simple language for ease of understanding.
NCERT CBSE Chapter 14 Breathing and Exchange of Gases Solutions of class 11 explains the mechanism of breathing, the exchange of gases, how the respiratory system is regulated, and the various disorders of the respiratory system. Revise the basic concepts of Breathing and Exchange of Gases for quick revision and class notes.
Q1: Define Vital Capacity. What is its Significance?
Answer:
Vital capacity is defined as the maximum volume of air a person can inhale after a forced expiration. This includes expiratory reserve volume, tidal volume, and inspiratory reserve volume. It is about 3.5-4.5 L.
The significance of vital capacity is that it promotes the intake of the maximum amount of fresh air and gets rid of foul air, thereby increasing the gaseous exchange between the tissue and the environment. This leads to an increase in the amount of energy available for various functions of the body.
Q2: State the Volume of Air remaining in the Lungs after normal Breathing.
Answer:
The volume of air remaining in the lungs after normal breathing can be stated by functional residual capacity (FRC). It is defined as the volume of air that will remain in the lungs after normal expiration. This includes expiratory reserve volume(ERV) and residual volume(RV).
Expiratory reserve volume(ERV) is defined as the additional volume of air, a person can exhale after forceful expiration. It is about 1000-1100 ml. Residual volume is defined as the volume of air that remains in the lungs after forceful expiration. It is about 1100- 1200ml. Hence,
FRC= ERV + RV = 1200+1100 = 2300
Therefore, the functional residual capacity is about 2200-2300ml.
Q3: Diffusion of Gases occurs in the Alveolar region only and not in the other parts of the Respiratory System. Why?
Answer:
The exchange of gases takes place when the respiratory surface has certain features like a thin surface, good blood supply, and a large surface area. Alveoli are small air sacs covered by a thin epithelial membrane. Its thickness is less than one millimetre. Being highly vascularised and irregularly shaped (that increases the surface area for the exchange of gases), alveoli form the primary site for the exchange of gases.
Q4: What are the major Transport Mechanisms for CO2? Explain.
Answer:
Every 100 ml of deoxygenated blood delivers approximately 4 ml of CO2 to the alveoli. The major transport mechanism for CO2 are:
- Transport of carbon dioxide as carbamino-haemoglobin.
About 20-25% of CO2 is carried as carbamino-haemoglobin. Partial pressure determines the binding of CO2 to haemoglobin. When pCO is high, and O2 is low( as in tissues), more binding of CO2 takes place. When the pCO2 is low, and pO2 high as in the alveoli, dissociation of CO2 from carbamino-haemoglobin takes place. Finally, the CO2 bound to haemoglobin from the tissue is released at the alveoli.
- Transport of carbon dioxide through plasma.
Nearly 5-7% of carbon dioxide is transported in a dissolved state through plasma.
- Transport of carbon dioxide as bicarbonate ions.
The partial pressure of CO2 is high in the tissues due to catabolism. CO2 diffuses into the blood and forms HCO–3 and H+. This reaction is facilitated by the carbonic anhydrase enzyme. pCO2 is low at the alveolar site, the reaction reverses and leads to the formation of CO2 and H2O. Hence, CO2 at the tissue level in the form of bicarbonate ions, is transported and released at the alveolar site as CO2. Nearly 70% of CO2 is transported as bicarbonate ions.
Q5: What will be the pO2 and pCO2 in the Atmospheric Air compared to those in the Alveolar Air?
- pO2 lesser, pCO2 higher
- pO2 higher, pCO2 lesser
- pO2 higher, pCO2 higher
- pO2 lesser, pCO2 lesser
Answer:
The pO2 and CO2 in the atmospheric air compared to those in the alveolar air will be (ii) pO2 higher, pCO2 lesser
pO2 in atmospheric air is about 159 mm Hg and in the alveolar air, it is about 104 mm Hg. So, pO2 is higher in atmospheric air than alveolar air. In atmospheric air, the pCO2 is 0.3 mm Hg and in alveolar air, it is 40 mm Hg, which means pCO2 in atmospheric air is less than pCO2 in alveolar air.
Q6: Explain the process of Inspiration under Normal Conditions.
Answer:
The process of inspiration under normal conditions takes place when the pressure within the lungs is less than the atmospheric pressure. It starts with the contraction of the diaphragm which increases the volume of the thoracic chamber in the anteroposterior axis. External intercostal muscles contracts and lifts up the ribs and sternum. It increases the volume of the thoracic chamber in the dorsoventral axis. The pulmonary volume increases after the increase in the thoracic volume, which decreases the intra-pulmonary pressure to less than the atmospheric pressure. The negative pressure that is created inside forces the air from outside to move into the lungs, completing the process of inspiration.

Q7: How is Respiration regulated?
Answer:
The respiratory rhythm centre located in the medulla region is primarily responsible for the regulation of respiration. The pneumotoxic centre located in the pons moderates the function of the respiratory rhythm centre. Signals from this centre reduce the inspiration. The chemosensitive area, aortic arch, and carotid artery are sensitive to CO2 and H+ concentrations. Change in the concentration of these substances sends signals to the rhythm centre to make necessary adjustments.
Q8: What is the Effect of pCO2 on Oxygen Transport?
Answer:
pCO2 plays a significant role in the transport of oxygen. When the pCO2 is low, as in the alveoli, O2 binds with the haemoglobin and forms oxyhaemoglobin. When is high, as in the tissue and pO2 is low, it results in the dissociation of O2 from oxyhaemoglobin. Hence, the affinity of haemoglobin for O2 increases when pCO2 is low. Therefore, O2 is transported as oxyhaemoglobin, and it dissociates at the tissues.
Q9: What happens to the Respiratory process in a man going Up a hill?
Answer:
As we go up the hill, the air becomes thin, and the atmospheric pressure and the oxygen content of the air decrease. Therefore, as the man goes up a hill, he will experience oxygen deficiency. This will result in low oxygen levels in the blood. To compensate for the decreased oxygen level in the blood, the respiratory rate increases along with the increase in the heart rate to supply more oxygen to the blood.
Q10: What is the site of Gaseous Exchange in Insects?
Answer:
Insects have a network of tubes that is a tracheal system to transport atmospheric air within the body. Air rich in oxygen enters through the spiracles, which are small openings on the side of the insect’s body. From the spiracles, the air reaches the trachea and is the diffused cell of the body.
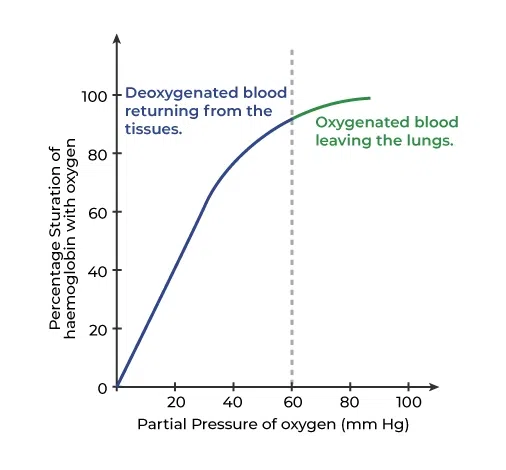
Q11: Define the Oxygen Dissociation curve. Can you suggest any reason for its Sigmoidal Pattern?
Answer:
The oxygen dissociation curve is defined as the curve obtained when the percentage saturation of haemoglobin with oxygen is plotted against the pO2. This curve is sigmoid in shape and is useful in studying the effects of factors like pCO2, and H+ ion concentration on the binding of O2 with haemoglobin. The dissociation curve is sigmoid because of the following reasons:
- When the first molecule of oxygen binds to the haemoglobin, the affinity of the second molecule increases, resulting in the rapid formation of oxyhaemoglobin. Graphically this is represented as a steep s-shaped slope.
- The curve becomes flat when the formation of oxyhaemoglobin stops.
Q12: Have you heard about Hypoxia? Try to gather information about it, and discuss it with your friends.
Answer:
Hypoxia is a condition when there is an inadequate supply of oxygen to the body tissues. It can be caused due to various reasons such as lung disease, heart problems, high altitudes, etc. The various types of hypoxia are:
- Hypoxic hypoxia: caused due to decrease amount of oxygen in the arterial blood.
- Anemic hypoxia: caused due to decrease in oxygen carrying capacity of the blood.
- Circulatory hypoxia: caused when there is inadequate blood flow to the tissues.
- Histotoxic hypoxia: caused when oxygen is available to the cells, but they are unable to use it. The symptoms of hypoxia are shortness of breath, increased heart rate, lethargy, anxiousness, etc.
Q13: Distinguish between
- (a) IRV and ERV
- (b) Inspiratory capacity and Expiratory capacity
- (c) Vital capacity and Total lung capacity
Answer:
|
IRV
|
ERV
|
|
Inspiratory reserve volume(IRV) is defined as the additional volume of air that can be inhaled by a forcible inspiration.
|
Expiratory reserve volume is defined as the additional volume of air that can be exhaled by a forcible expiration.
|
|
It is about 2500ml – 3000ml.
|
It is about 1000ml – 1100ml.
|
- (b)Inspiratory capacity and Expiratory capacity
|
Inspiratory capacity
|
Expiratory capacity
|
|
Inspiratory capacity is defined as the total volume of air that can be inhaled after a normal expiration.
|
Expiratory capacity is defined as the total volume of air that can be exhaled after a normal inspiration.
|
|
Inspiratory capacity is the sum of tidal volume and inspiratory reserve volume (TV+IRV).
|
Expiratory capacity is the sum of tidal volume and expiratory reserve volume (TV+ ERV).
|
- (c) Vital capacity and Total lung capacity
|
Vital capacity
|
Total lung capacity
|
|
Vital capacity is defined as the total volume of air, we can breathe in after forced expiration.
|
Total lung capacity is defined as the total volume of air accommodated in the lungs, at the end of forced inspiration.
|
|
Vital capacity includes Inspiratory reserve volume, tidal volume, and expiratory reserve volume. (IRV, TV, ERV).
|
Total lung capacity includes reserve volume, expiratory reserve volume, tidal volume, and Inspiratory reserve volume.
|
Q14: What is Tidal volume? Find out the Tidal volume (approximate value) for a healthy human in an hour.
Answer:
Tidal volume is defined as the volume of air inhaled or exhaled during normal respiration. It is about 500 ml. A healthy man can inhale or exhale approximately 6000 – 8000ml of air per minute. Therefore, the tidal volume of a healthy human in an hour will be approximately can be 3,60,000 ml – 4,80,000 ml.
Like Article
Suggest improvement
Share your thoughts in the comments
Please Login to comment...